The introduction to Solihull (Draft) Infrastructure Delivery Plan (IDF) explains it ‘…is a key component of the evidence base to support the Local Plan. The IDP provides a baseline of the existing infrastructure capacity and needs in the Borough and highlights the infrastructure requirements to support the predicted growth set out in the Local Plan.’
The IDP provides a snapshot at the time of publication. Continuing that over the lifetimes of the plan period ‘new funding opportunities will arise, equally, infrastructure priorities may change. And that the IDP will be reviewed on an annual basis subsequent to Adoption.
The IDP can be found below, but I have provided some context about Health provision that I feel has great importance:
HEALTH: Access to Primary Care is problematic for many people and IT is a very fair and appropriate question on the doorstep ‘How can you build more homes when we can not get doctors’ appointments now?’
The IDP refers to Health concerns and the identified need for more provision in paragraph 4.3.1 (page 81 onwards). I have though summarised them below. As we move towards the likelihood of large planning applications coming before planning committee for determination I believe it is vital we review the requirements for Health and Community provision within the IDP sooner rather than later and I have requested our officers to undertake this.
Underpinning this is the council’s Planning Policy P21, which refers to ‘Delivery and Infrastructure and securing developer contributions for new infrastructure required as a result of development.’
The Council have been working with the NHS and Clinical Commission Group (CCG) to determine the impacts of the new population growth on the Borough’s health services. The CCG have provided overarching figures on new requirements as a result of the additional population. These were produced prior the Covid 19 pandemic taking effect and the demand on primary care especially has risen dramatically. It is therefore important data is reviewed.
Between the period 2020-2036, it had been estimated that the following will be required by 2036, based on current levels of healthcare utilisation for the projected age cohorts:
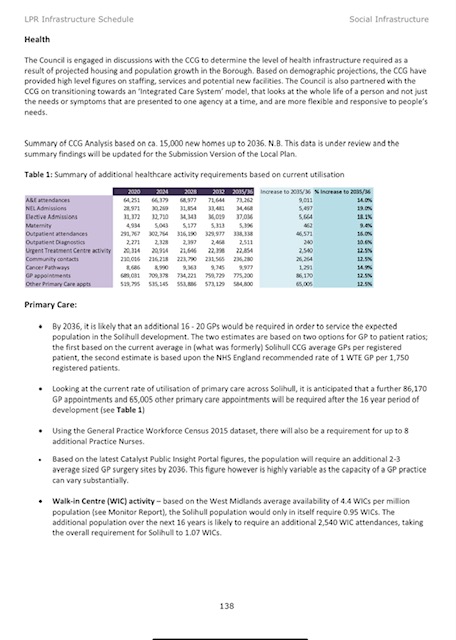

The above table (table 1) explains that by 2036, it is likely that an additional 16 – 20 GPs would be required in order to service the expected population in the Solihull development. The two estimates are based on two options for GP to patient ratios; the first based on the current average in (what was formerly) Solihull CCG average GPs per registered patient, the second estimate is based upon the NHS England recommended rate of 1 WTE GP per 1,750 registered patients.
Looking at the current rate of utilisation of primary care across Solihull, it is anticipated that a further 86,170 GP appointments and 65,005 other primary care appointments will be required after the 16-year period of development (see Table 1).
Conclusion:
As you will find, a great deal of work has gone into preparing for the needs of the borough following the implementation of house building resultant from the local development plan (which is still to be adopted). Some issues may not need revising much, identified highway infrastructure needs for instance. However, access to health provision, both primary and secondary care is a valid concern and no major housing development should be determined without an updated plan as to how existing and new residents of the borough will be cared for. I do not feel we need to know detailed plans but do deserve an outline as to where new medical practices will likely be centred to accommodate the new demand.

3 thoughts on “SOLIHULL – INFRASTRUCTURE DELIVERY PLAN”